0
Skip to Content
Calendar / Calendario
Beliefs / Creencias
Meeting Times / Horarios de Reunión
Our Team / Nuestro Equipo
Donate / Donar
Open Menu
Close Menu
Calendar / Calendario
Beliefs / Creencias
Meeting Times / Horarios de Reunión
Our Team / Nuestro Equipo
Donate / Donar
Open Menu
Close Menu
Calendar / Calendario
Beliefs / Creencias
Meeting Times / Horarios de Reunión
Our Team / Nuestro Equipo
Donate / Donar
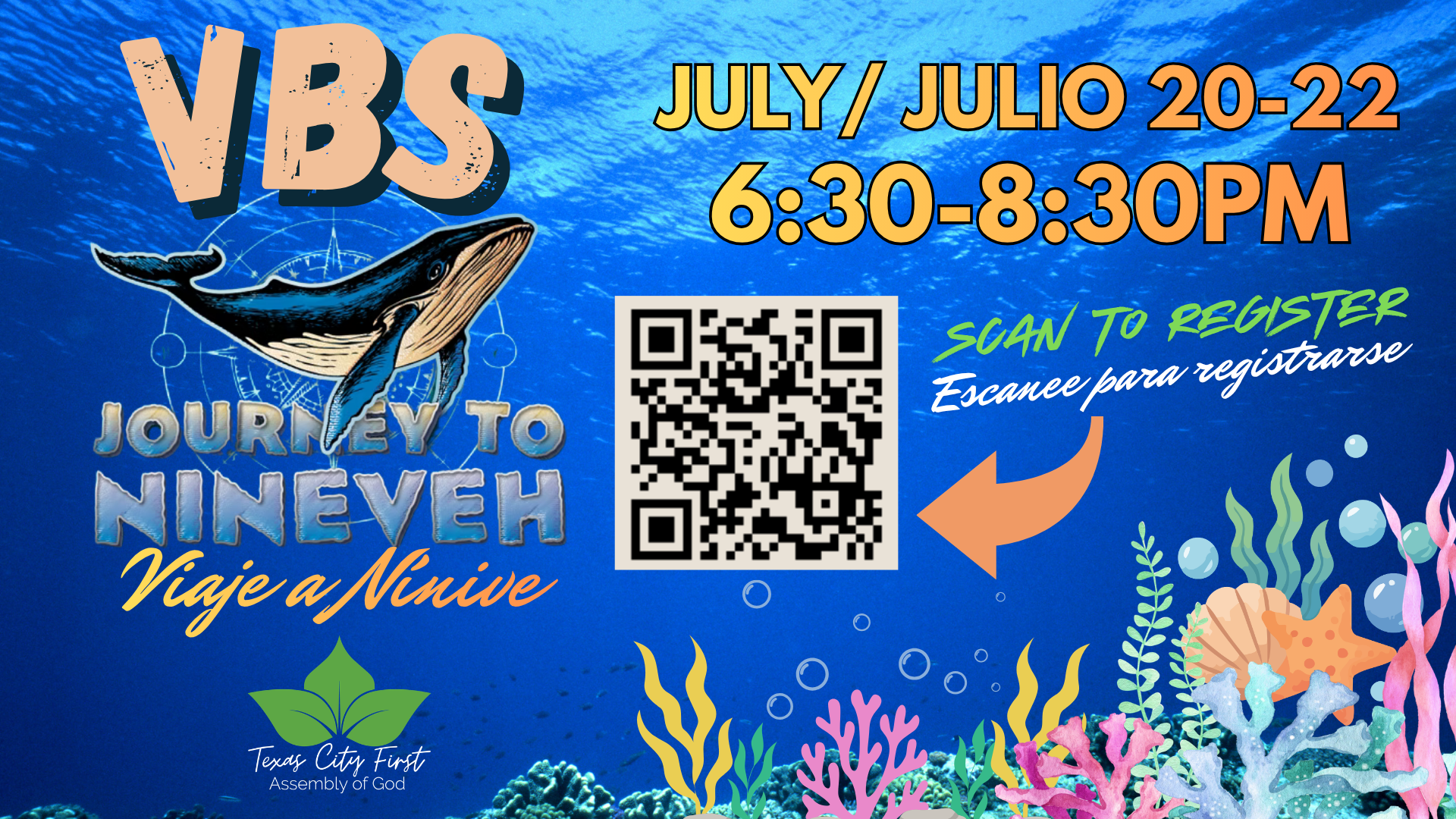
VBS Activity Consent Below / Consentimiento para la actividad del VBS a continuación